 Electrosurgery can, and does, create surgical smoke which may have several effects even during laparoscopic surgery.
Electrosurgery can, and does, create surgical smoke which may have several effects even during laparoscopic surgery.
Three primary issues associated with surgical smoke created by electrosurgery plague the operating room, those being odor, particulate matter and viable organisms. We should consider the unpleasant odor a warning of the damages the other issues can cause. Particulate matter interferes with the visual field of the surgeon, causes respiratory issues for the people in the room and can even clog suction lines. Even after the discovery that airborne materials could infect staff members, we had not fully realized all of the dangers to the patient.
During laparoscopic procedures the smoke created can, and often does, impair the surgeon’s visualization of the surgical field. This makes the observation difficult and can cause delays in completing the procedure.
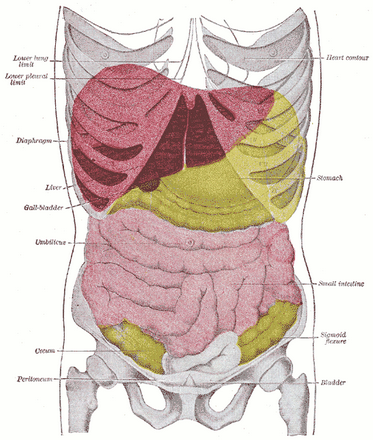
Perhaps the most disturbing fact is that the smoke that builds up inside the patient’s abdomen during laparoscopy can pass through the peritoneal membrane. As the red blood cells absorb the smoke, carboxyhemoglobin and methemoglobin increases, depleting the oxygen carrying capacity of the red blood cells. Further complicating the issue is that when we evacuate the surgical smoke from the abdomen, we also evacuate the carbon dioxide used to distend the abdomen for surgery. In order to maintain an adequate visual field, we must establish a method of replacing the carbon dioxide lost during the evacuation process. Further, when we place the evacuation tube, the pressure behind the pneumoperitoneum quickly forces the gas into the room. The solution is careful regulation of the evacuation.
Hoses designed for laparoscopic procedures need to be fitted with a valve or cannula stopcock. The surgical staff can then gradually evacuate the surgical smoke as they replenish the CO2 in the pneumoperitoneum. The evacuated smoke should then pass through a filtration system before re-entering the room.
Recognizing the necessity of surgical smoke management and evacuation, the next issue is how best to accomplish it. The primary considerations are:
- Ease of use - needs to be easy to use and maintain for optimal efficiency
- Noise level - must be quiet and not disruptive to the surgical routine
- Foot pedal activation or an automatic on and off sensor - so that the unit does not require significant action to operate
- Accessibility and portability - important when the unit moves between multiple locations
- Indicator light - signals the need to change the filter so that the system is always ready for use
- Efficiency - the unit must provide the smoke evacuation necessary for a clear surgical field and safe environment for both patient and surgical staff.
- Cost - should be economical to acquire and operate
The efficiency of the unit is the most critical factor. The motor rating of the evacuator, the tubing size and the proximity of the collection tubing to the surgical site all affect the quantity of smoke collected. The system should feature a triple filter system including a filter to collect larger particles, an ultra-low penetration air filter to capture smaller particles and a charcoal filter for toxic gas and odor absorption. Coconut-based charcoal filters are most efficient for gas and odor.
Bovie Medical Corporation offers effective surgical smoke elimination via the Smoke Shark II. It is compact and lightweight for easy storage and portability. Both the SF35 Extended-Life Filter and the FSSEP Pneumatic Footswitch are included with the SE02 unit. The filter performs effectively for approximately 35 hours, representing a procedure cost reduction of 38 percent when compared to the original Smoke Shark. The 3-port filter accommodates tubing sized one-fourth inch, three-eighths inch, and seven-eighths inch. The operating staff will appreciate the quiet levels of operation the Smoke Shark II affords. Contact a Bovie Medical representative for more information.


Image: http://upload.wikimedia.org/wikipedia/commons/4/43/Gray1224.png
{kind=link}